
Page 41 - Benefits-Guide-2020
P. 41
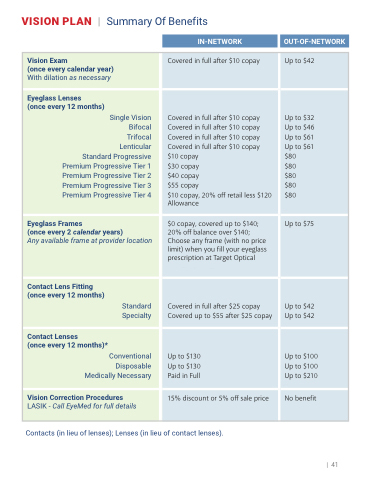
VISIONPLAN | SummaryOfBenefits
IN-NETWORK OUT-OF-NETWORK
Vision Exam
(once every calendar year) With dilation as necessary
Covered in full after $10 copay
Up to $42
Eyeglass Lenses
(once every 12 months)
Single Vision Bifocal Trifocal Lenticular Standard Progressive Premium Progressive Tier 1 Premium Progressive Tier 2 Premium Progressive Tier 3 Premium Progressive Tier 4
Covered in full after $10 copay Covered in full after $10 copay Covered in full after $10 copay Covered in full after $10 copay $10 copay
$30 copay $40 copay $55 copay
$10 copay, 20% off retail less $120 Allowance
Up to $32 Up to $46 Up to $61 Up to $61 $80
$80 $80 $80 $80
Eyeglass Frames
(once every 2 calendar years)
Any available frame at provider location
$0 copay, covered up to $140; 20% off balance over $140; Choose any frame (with no price limit) when you fill your eyeglass prescription at Target Optical
or Sears Optical
Up to $75
Contact Lens Fitting (once every 12 months)
Standard Specialty
Covered in full after $25 copay Covered up to $55 after $25 copay
Up to $42 Up to $42
Contact Lenses
(once every 12 months)*
Conventional Disposable Medically Necessary
Up to $130 Up to $130 Paid in Full
Up to $100 Up to $100 Up to $210
Vision Correction Procedures
LASIK - Call EyeMed for full details
15% discount or 5% off sale price
No benefit
Contacts (in lieu of lenses); Lenses (in lieu of contact lenses).
| 41
